Converting Waste to Value
Recycling is not the challenge.

Recycling is not the challenge.

Improperly irrigated land has led to low income and food insecurity.



A new perspective

The world is not on track, and more off track than four years ago

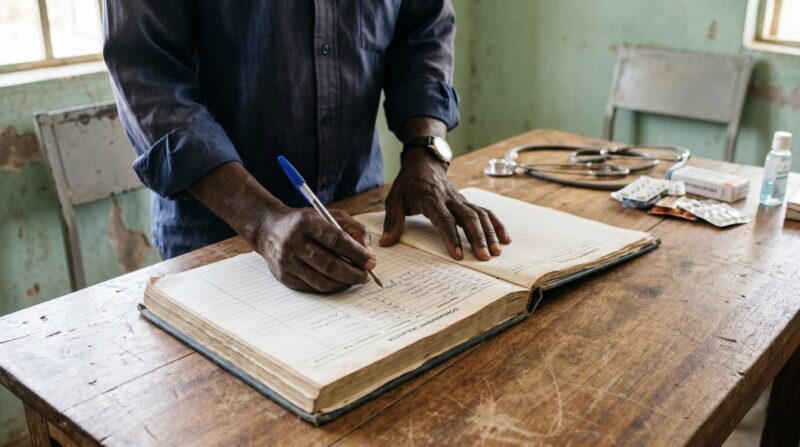
Community health workers often form the first and most consistent point of contact between underserved communities and the health system.
Nigeria receives billions in diaspora remittances each year, yet only a small share is directed toward health. Nzube Ifediba argues that diaspora capital could play a catalytic role in strengthening Nigeria’s strained health workforce — not by trying to replace migrating doctors and nurses, but by supporting the community health workers already closest to underserved populations.
The recent FP Analytics and Ford Foundation report on Nigeria’s diaspora philanthropy ecosystem confirms what has become increasingly clear: diaspora remittances represent one of the most significant sources of capital flowing into the country. They far outpace official development assistance and are likely to become even more important as donor commitments to foreign aid continue to weaken. In 2024 alone, remittances to Nigeria reached nearly $21 billion — considerably more than ODA in the same year. Across Africa, the pattern is similar: over the last two decades, remittances have exceeded foreign direct investment and ODA combined.
Yet Nigeria’s diaspora giving remains disproportionately concentrated. Over a five-year period, for example, 87.5% of UK diaspora remittances for infrastructure went to private housing, while just 1.8% went to health. If remittances have such transformative potential, the question is not only how much money is flowing back to Nigeria, but whether some of that capital can be more intentionally directed toward social systems and the SDGs.
Nigeria’s health workforce is one urgent place to start. With 3.9 doctors and 15.6 nurses per 10,000 people — well below the WHO-recommended threshold — the system is already strained. Migration is making the challenge worse: 42,000 nurses have reportedly left Nigeria in the last three years, more than 9,000 doctors have migrated, and surveys suggest that a large share of the remaining health workforce is considering leaving.
Diaspora health workers are often proposed as part of the solution, through remittances, skills transfer, training, and capacity building. These contributions matter. But my own rapid review found that remittances from diasporan skilled health workers rarely reach the poorest Nigerians, who are often the most vulnerable to health workforce loss. Skills transfer is also valuable, but it cannot match the scale of the manpower deficiency.
What if, then, Nigeria’s diaspora health workers and philanthropists began not by trying to replace the skilled health workers who have left, but by strengthening the community health workforce already closest to the people most affected?
Community health workers offer a more scalable and tractable starting point.
While there are no hard estimates, community health workers are widely understood to be the largest workforce in Nigeria’s public primary health care system. In the literature, they are often regarded as the first point of contact in public primary health centres, especially in remote and rural areas. They are also frequently used to fill gaps left by shortages of physicians and nurses.
This makes community health workers central to the everyday functioning of primary care. They use local knowledge, trust, and grassroots engagement to support primary prevention, immunization, disease surveillance, maternal and child care, and other essential services. In communities where doctors and nurses are scarce, they are often the health system’s most visible and consistent presence.

Diaspora capital could help strengthen the frontline health infrastructure that many rural and underserved communities already depend on.
They are also comparatively fast to train. Community health worker training typically takes one to three years, far less time than the training required for doctors, nurses, and other skilled health professionals. Because their work is concentrated at the primary care level, investments in this workforce also align with some of the most cost-effective health interventions available.
The case, then, is not that Nigeria should ignore secondary and tertiary health systems. It is that a diaspora capital strategy focused only on doctors, nurses, and specialist skills will miss one of the most immediate opportunities to strengthen access, prevention, and continuity of care for the most vulnerable populations.
Despite their importance, many community health workers in Nigeria remain structurally neglected.
Formal cadres, including Community Health Officers and Community Health Extension Workers, are technically salaried. But even they can struggle to receive consistent pay because of local government funding gaps, administrative delays, and weak payroll reliability. Below them, CHIPS Agents and Volunteer Community Mobilisers are often unpaid, receiving only small stipends intended to cover transport or basic operating costs.
This is particularly striking because these workers are among the most frontline-facing members of the health system in remote and underserved communities. They are asked to deliver preventive care, encourage immunization, monitor local health risks, and support maternal and child health — often without the professional recognition, remuneration, or career pathways that would make their work sustainable.
That neglectedness is where diaspora capital could play a catalytic role.
There is room for diaspora capital to support Nigeria’s community health workforce through both philanthropic and commercial vehicles. None of these models is simple, and each would require careful design, strong governance, and credible impact measurement. But together they point toward a more intentional use of diaspora resources for health-system strengthening.
The most practical starting point may not be the most visible professionals, but the most proximate ones: community health workers.
One possibility is an outcomes-based financing model. Diaspora investors could provide upfront capital for community health worker interventions, with repayment tied to measurable outcomes such as improved immunization coverage, reduced maternal mortality, better disease surveillance, or decreased avoidable hospital admissions. In theory, such a model could reduce upfront fiscal pressure on government while attracting co-financing from development finance institutions.
Nigeria already has experience with results-based financing for primary health centers, primarily through conditional grants from DFIs. Diaspora capital could potentially complement those flows, especially where upfront investment helps unlock additional funding and creates a dedicated pool for community health worker remuneration.

The challenge is not simply attracting more capital, but designing financing mechanisms that strengthen access, accountability, and continuity of care.
A more ambitious model would be a revenue-generating public-private partnership, in which diaspora investors help finance or co-own primary health centers in partnership with government. In such a model, facilities might combine government capitation payments, community insurance arrangements, and modest subscription-based revenue to create a more reliable basis for paying community health workers directly.
But this model also carries real risks. Purchasing power is limited in rural Nigeria, where health needs are often greatest and incomes lowest. Any revenue-generating approach would need safeguards to ensure that poor households are not priced out of essential care. If diaspora capital is to support primary health infrastructure, it must strengthen access rather than reproduce the exclusions that already weaken the system.
At the most direct end of the philanthropic spectrum are grants. Diasporans could provide one-off or recurring grants to community health workers serving in remote or underserved facilities. This approach is less complex than impact bonds or PPPs, and its additionality case is strong: these are workers least likely to receive reliable government salary payments, least visible to institutional donors, and most dependent on informal community support.
Small, predictable investments in frontline workers can have outsized effects on retention, morale, and service delivery.
The key point is not that cash transfers alone can solve Nigeria’s health workforce crisis. Rather, direct support to community health workers may be one of the few ways diaspora philanthropy can reach the exact layer of the system where small, predictable payments could have immediate effects on retention, morale, and service delivery.
The larger challenge is sustainability. Diaspora grants and investment vehicles can help fill urgent gaps, but community health workers cannot remain dependent on episodic generosity. If they are essential to Nigeria’s health system, they should eventually be treated as part of its core public infrastructure.
Liberia offers a useful proof of concept. Before 2016, the country relied on a fragmented system of unpaid volunteers across several cadres. After the Ebola epidemic, the government institutionalized a paid, professional community health worker cadre through the Revised National Community Health Services Policy of 2016. Community health workers were placed on the government payroll, with funding support from international donors.
Diaspora capital must strengthen access rather than reproduce the exclusions that already weaken the system.
Nigeria’s context is different, and the model cannot simply be imported. But Liberia’s experience shows that unpaid or semi-formal community health labor can be professionalized when political will, donor finance, and public-health priorities align. Diaspora capital could help create similar momentum in Nigeria by funding pilots, supporting remuneration, building evidence, and demonstrating the value of a more stable community health workforce.
Nigeria’s diaspora remittances are already reshaping households, communities, and local economies. The question is whether a portion of that capital can also help strengthen the social systems on which those communities depend.
For Nigeria’s health workforce crisis, the most practical starting point may not be the most visible professionals, but the most proximate ones: community health workers. Strengthening them would not solve every health-system challenge. But it could improve primary care, reach underserved populations, and offer diaspora philanthropists and investors a high-leverage way to support the people already holding together the first line of care.


Related Content

Transforming agriculture to incentivize climate resilience

An urgent call for intentional design and transparent governance

Comments

Deep Dives
RECENT



Editor's Picks



Webinars
News & Events
Subscribe to our newsletter to receive updates about new Magazine content and upcoming webinars, deep dives, and events.
Become a Premium Member to access the full library of webinars and deep dives, exclusive membership portal, member directory, message board, and curated live chats.

Join our global community of systems-minded changemakers.
Subscribe to the Impact Entrepreneur newsletter for the latest insights, magazine features, and invitations to exclusive webinars, Deep Dives, and events.


0 Comments